

How bad will winter get?
How bad will winter get?
Healthcare in the northeast might be heading for disaster

The bad cat has already detailed how cases are climbing in northern states at a rate far surpassing what was seen last year, in spite of, and, worryingly, possibly due to the extremely high vaccination rates among vulnerable and adult populations in that part of the country. As the weather gets colder and we hit peak season, the numbers of cases, hospitalizations, and deaths could be (relatively) astronomical.
(Note the case fatality rate is still expected to be less than 1%, but deaths could still easily exceed last winter’s number by an order of magnitude even before considering the mess that might be NE hospitals in the coming months)
Some of the bigger cities haven’t handled seasonal surges in the best of times. But what happens when they start that surge short staffed as they insist on driving away health care workers?

Those mandates were hitting the southeast around the same time with some disastrous consequences. Alabama had to scrap the whole thing, after they hit 100% ICU capacity. This was in part because of a seasonal spike in hospital admittance, but mostly because they didn’t have the personnel to staff ICU beds. Hospitals are supposed to have the flexibility to expand available beds on short notice, but they can’t do it if they just fired all their nurses.

Seasonality might have given a lot of cover to bad policies. Sure, ICUs were at capacity, but that was because of the unvaccinated. There’s no way the same thing could happen in New York, right? Make no mistake about it, plenty of hospital systems in the north are critically low on manpower, but in the offseason, it doesn’t look like a disaster.
On top of what might be a powder keg, we might be getting ready with a lit match. The CDC has gone ahead with a recommendation for boosters for all healthy adults. If Gato’s vaccinated superspread hypothesis is correct (absolutely still just a hypothesis at this point, but a persuasive one), what are fall boosters going to do to the numbers? As he documents, the lack of sterilizing immunity and higher susceptibility in the weeks following the first (or third) dose seems to correspond to a spike in cases. This spike can get lost in the noise when out of season or coming down off a seasonal peak, but if a big booster program starts right as you are coming into season, especially in a population that has shown a readiness to follow guidelines, you can get an explosion in cases.
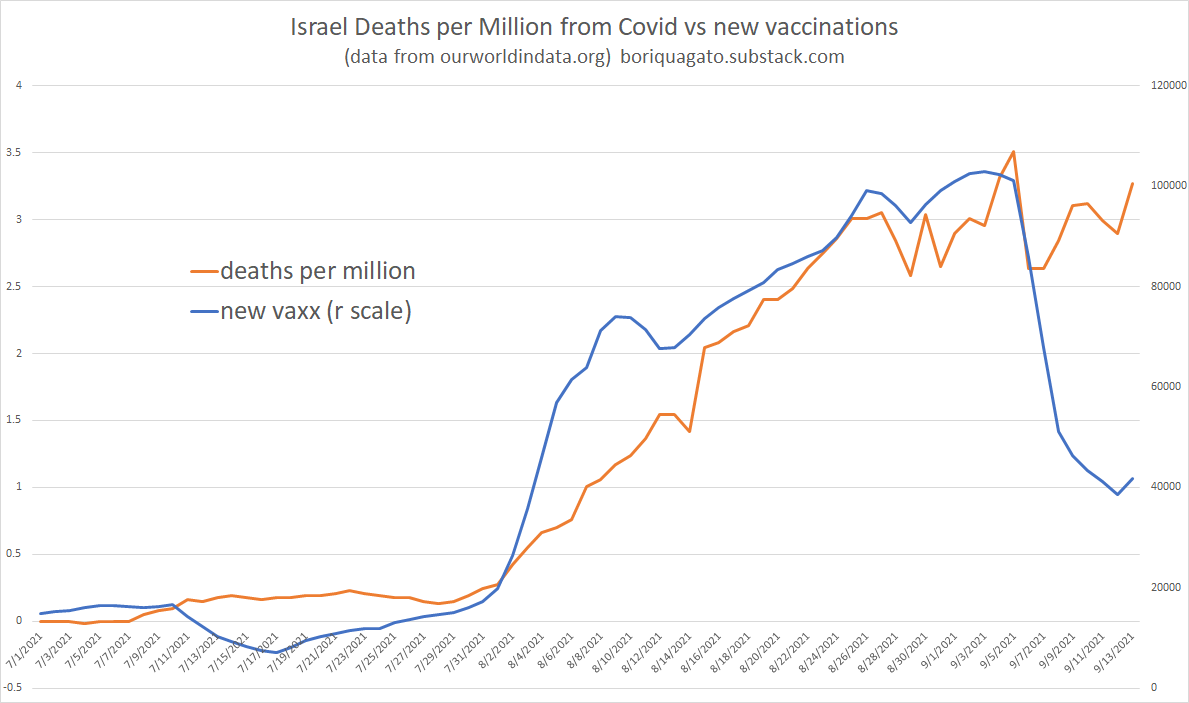
And not just cases either. In Israel, the country that has been most aggressive in administering boosters, deaths has been rising in lock step with booster rates.
So what does all this mean for the winter. Assuming humans up north are the same way as the rest of the world, the seasonal spike is going to dwarf anything they saw last year, they are going to be admitted to hospitals who are in the process of cutting their staff by 10-20%, and they are going to be eager for boosters which appear to cause a lot of pain in the short term. Add to this that the powers that be are unwilling to admit mistakes, that all they know how to do is double down of failed policies, and we might be heading for a generational failure in healthcare.
Well, that was cheery.